Children's care
Guiding your child's jaw, airway, and breathing development from the very start.
When growth is still active, gentle, well-timed assessment can work with development rather than against it.
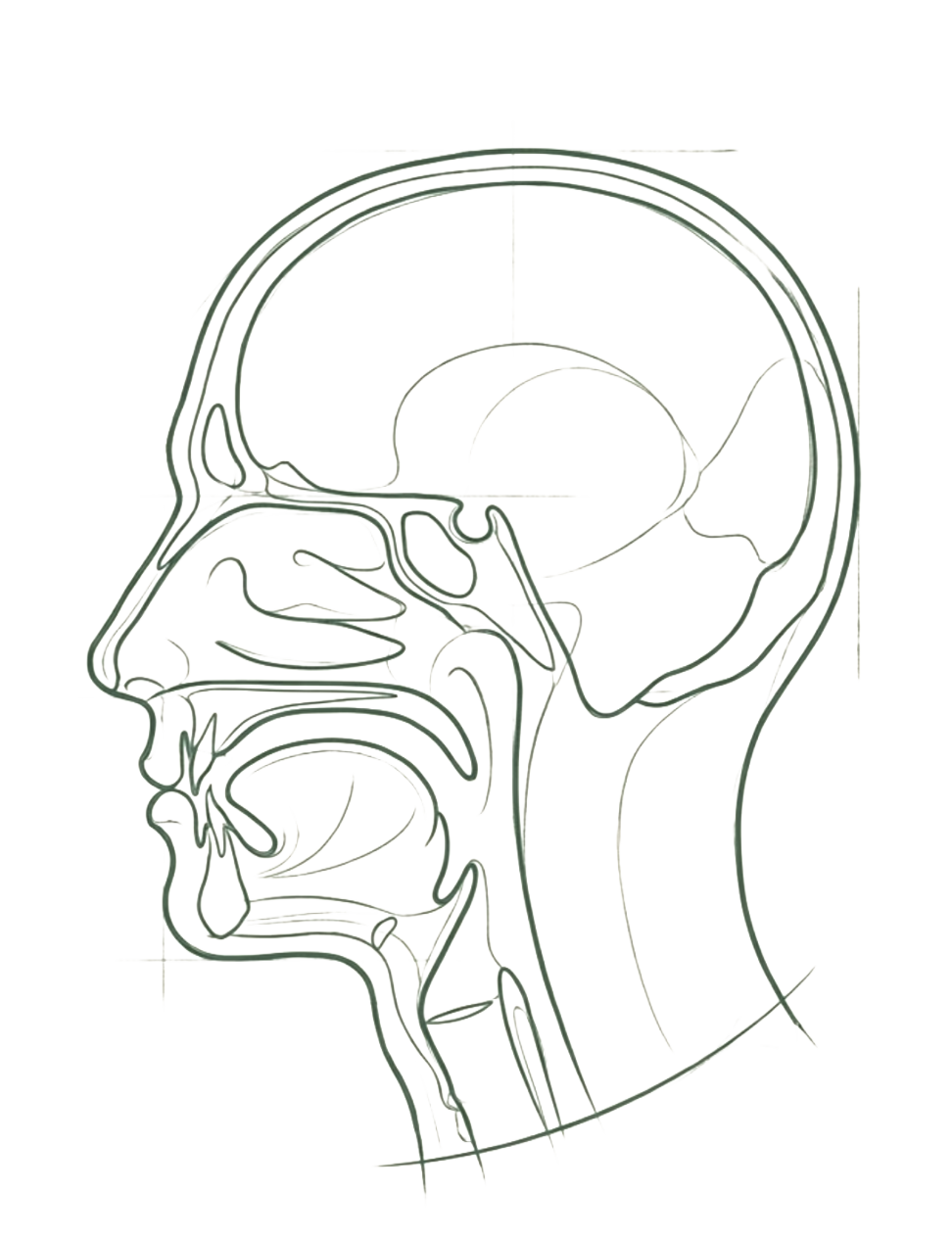
A child's face, jaw, and airway do not simply grow on a fixed schedule. They respond to function. The way a child breathes, swallows, and holds their tongue at rest all shape how the bones of the face and jaw develop over time. This is not a permanent window, but it is a meaningful one. The years between ages four and twelve represent a period of significant skeletal plasticity, when gentle, well-timed intervention can work with natural growth rather than against it.
Breathing through the nose, with the tongue resting against the palate, encourages the upper jaw to widen and the airway to develop with adequate space. When that pattern is disrupted, by mouth breathing, a restricted tongue, or poor oral muscle function, the resulting structural changes can become increasingly difficult to address with age. Assessing how these systems are working together, early, can make a meaningful difference to the path ahead.
Parents are often the first to notice something is off
Children rarely report breathing difficulties. Some signs can be subtle; others are easier to spot. Seen together, across three areas, they are worth assessing.
01 Breathing & sleep
- Breathing through the mouth, particularly during sleep or at rest
- Snoring, restless sleep, or waking frequently through the night
02 Teeth & jaw
- Crowded, crooked, or irregularly spaced teeth as adult teeth come in
- A narrow upper jaw or high, vaulted palate
- A small lower jaw or recessed chin
03 Body & daytime
- Forward head posture or rounded shoulders
- Difficulty concentrating, irritability, or tiredness out of proportion to sleep hours
- Slow or fussy eating, or a tendency to chew with the mouth open
None of these signs on their own confirms a problem, but together they can point toward patterns worth assessing properly.
Early-stage orthodontics, sometimes called interceptive orthodontics, is not about straightening teeth for appearance. It is about addressing the structural and functional conditions that are causing teeth to crowd or the bite to develop incorrectly in the first place.
Traditional orthodontic treatment typically begins in the early teenage years, once most of the adult teeth have come through. At that stage, the objective is usually alignment. Early-stage orthodontics begins considerably sooner, during the mixed dentition phase when baby and adult teeth coexist, with the aim of supporting healthier jaw development before the growth window narrows.
This can involve gentle palatal expansion, addressing tongue and lip function, and guiding the eruption of adult teeth into better positions. The forces used are light and gradual, working in keeping with how children's bones naturally respond to low-level, sustained pressure.
Airway assessment at Growth and Airway goes beyond a visual examination. Using cone beam CT imaging where appropriate, it can be possible to evaluate the dimensions of the nasal and oral pharyngeal airway, identify potential obstructions such as enlarged tonsils or adenoids, and observe how tongue posture and oral muscle function are affecting available space.
The aim is to understand whether the airway is developing with enough room for healthy nasal breathing, and whether any structural or functional factors are interfering with that. Where relevant, this assessment connects with myofunctional therapy, breathing retraining, and, in some cases, referral to an ENT or other appropriate clinician.
Invisalign First is a clear aligner system designed specifically for younger children, typically between six and ten years of age. It can be used to gently widen the upper arch and create space for incoming adult teeth, without the need for fixed metal appliances.
For some children, Invisalign First can be a well-tolerated option, particularly where compliance is likely to be good. Like all orthodontic approaches, it works best when considered alongside the broader functional picture, including tongue function, breathing pattern, and oral muscle habits. Whether it is the right option for a given child is something that can be assessed properly at consultation.
An assessment, not a commitment to treatment
Parents leave the consultation with a genuine understanding of the situation, not a list of procedures.
A conversation
The first appointment typically includes a conversation about your child's sleep, breathing, eating habits, and medical history.
Clinical examination
A clinical examination of the teeth, jaw, bite, and oral muscle function follows, building a clear picture of what is and is not developing as expected.
Imaging where indicated
Where imaging is indicated, a cone beam CT scan can provide a three-dimensional view of the airway and facial structures.
Options in plain terms
Any options are explained in plain terms, so you leave with a genuine understanding of the situation rather than a list of procedures.
If something has caught your attention, an assessment is the right next step.
Book a children's consultation with Growth and Airway.